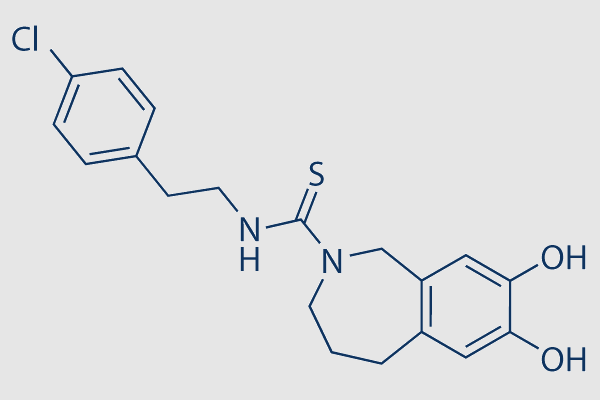
[CAS NO. 138977-28-3] Capsazepine
Please click "REQUEST A QUOTE" button if you need other sizes or custom synthesis
request a quote
If there is no stock, or you need other sizes or custom synthesis, please:
PRODUCTS SPECIFICATIONS [138977-28-3]
Store
Catalog
SLK-S8137
Brand
Selleck
CAS
138977-28-3
DESCRIPTION [138977-28-3]
Overview
| MDL | MFCD00153778 |
|---|---|
| Molecular Weight | 376.90 |
| Molecular Formula | C19H21ClN2O2S |
| SMILES | C(NCCC1=CC=C(Cl)C=C1)(=S)N2CC=3C(=CC(O)=C(O)C3)CCC2 |
For research use only.
Storage
3 years,-20°C,powder
1 years,-80°C,in solvent
1 years,-80°C,in solvent
Shipping
Room temperature shipping(Stability testing shows this product can be shipped without any cooling measures.)
Description
Capsazepine acts as a competitive antagonist of capsaicin and a antagonist. If you want to do cell experiments, please select batch 01.
In vitro
Capsazepine(CPZ) at a concentration of 94.2 µg/ml (IC50 concentration of capsazepine) exhibits a statistically significant inhibition of osteoclast growth and proliferation. Capsazepine converts the NKA into Na-ATPase. CPZ inhibits K+-dependent activity but allows Na-ATPase associated with Na+ transport. CPZ has no effect on Na-ATPase measured in the absence of K+. CPZ also inhibits para-nitrophenyl phosphatase activity, albeit with a lower affinity. CPZ strongly reduces the steady-state EP level and the Na+ affinity for phosphorylation decreased 3-fold after CPZ treatment. In summary, CPZ blocks an Na+/K+ cycle in the NKA but leaves an Na+ cycle intact, reducing the transport stoichiometry of the pump. Capsazepine inhibits osteoclast formation and bone resorption in a dose dependent manner in bone marrow-osteoblast co-cultures and RANKL generated osteoclast cultures. Capsazepine also suppresses RANKL induced IκB and ERK1/2 phosphorylation and causes apoptosis of mature osteoclasts and also inhibits alkaline phosphatase activity and bone nodule formation in calvarial osteoblast cultures.
In vivo
In mice, the TRPV1 antagonist capsazepine blocks morphine tolerance and dependence in mice. Acute capsazepine treatment (5 mg/kg, i.p.) potentiates the antinociceptive effects of morphine, as measured by the hot-plate test. Repeated co-treatment of capsazepine (2.5 mg/kg, i.p.) with morphine attenuates the development of tolerance to the antinociceptive effect of morphine. The development of morphine dependence is also reduced by capsazepine (1.25 or 2.5 mg/kg, i.p.). Capsazepine (1 mg/kg/day) inhibits ovariectomy induced bone loss in mice and histomorphometric analysis shows inhibitory effects on indices of bone resorption and bone formation.
References
Synonyms
2H-2-Benzazepine-2-carbothioamide, N-[2-(4-chlorophenyl)ethyl]-1,3,4,5-tetrahydro-7,8-dihydroxy-
N-[2-(4-Chlorophenyl)ethyl]-1,3,4,5-tetrahydro-7,8-dihydroxy-2H-2-benzazepine-2-carbothioamide
Capsazepine
Powered by Arctom Copyright © 2026 Arctom. All rights
reserved.